In this Medical Monday series, we’re talking about how your doctor reaches a diagnosis of common conditions associated with coagulation. It may help if you first read the introduction, before reading about today’s topic of heart attack. Altogether we’re covering
- Introduction
- DVT, Deep Vein Thrombosis
- Post-thrombotic syndrome
- PE, Pulmonary Embolism
- Pulmonary hypertension
- AF, Atrial Fibrillation
- Heart Valve conditions – aortic and mitral
- Thrombophilia
- Stroke
Your story
 The characteristic symptom of a heart attack is pain in the centre of the chest or upper abdomen (the epigastrium), this is the presenting feature in about three quarters of people.
The characteristic symptom of a heart attack is pain in the centre of the chest or upper abdomen (the epigastrium), this is the presenting feature in about three quarters of people.- The pain can stay localised to the centre of the chest, but it often spreads to the left arm or neck; less commonly it spreads to both arms, the shoulders or the jaw.
- The pain is described as pressure, like a heavy weight on the chest, one patient told me it felt like an elephant was sitting on his chest. However the pain is sometimes described as a squeezing, or aching sensation.
- The pain is often associated with sweating, nausea, and vomiting.
- Some people get short of breath or notice palpitations.
- Although we all have some idea of the common presentation from TV shows and movies it is important to know that in about a quarter of patients the symptoms can be quite different. There may be no chest pain but just pain in the jaw or in the middle of the abdomen. In some cases there is virtually no pain, there may be sudden onset of an abnormal heart rhythm or sudden shortness of breath. In older people acute onset of confusion may be the only symptom. Atypical presentations are more common in women, older men, people with diabetes and people from asia.
This video gives a realistic idea of a common presentation
Questions your doctor may ask
Chest pain is always taken very seriously by your doctor. Your doctor will want to know when the pain started, the nature of the pain and if it radiates anywhere else in your body, particularly to your arm or neck. Most people having a heart attack feel very unwell, nausea and sweating are common. Urgent treatment may be required so your doctor will refer you to hospital immediately if a heart attack is suspected. However there are many causes of chest pain that doctors see everyday. Many people with chest pain are worried they are having a heart attack but the cause of the pain is often something far less serious.
If you are referred to hospital, the doctors are likely to ask you about any risk factors you may have such as high blood pressure, a history of smoking, a high cholesterol, diabetes or a family history of heart disease. They will want to know about any previous history of angina or heart disease and what medication you are taking. They may also want to know if you are on an anticoagulant or have a history of bleeding as they may be considering giving you treatment to break down the blood clot causing the heart attack; this treatment is called thrombolysis.
What your doctor may find

There can be a wide range of findings.
- Patients often look pale with cold clammy skin.
- The pulse rate can be slow in some cases but in others it is very fast and the blood pressure can sometimes be high and in other cases low, depending on the size of the heart attack.
- When your doctor listens to your heart he may hear nothing abnormal, but sometimes there are extra heart sounds due to strain on the heart. If the heart attack has affected a heart valve or affected the ability of the heart to pump properly there may be a new heart murmur present, and in some cases a heart attack can cause inflammation of the covering of the heart and the doctor might hear a sound called a pericardial rub; it sounds a bit like a squeaky shoe.
- Your doctor may also hear some crackling sounds in your chest due to increased fluid in your lungs.
Tests you may have
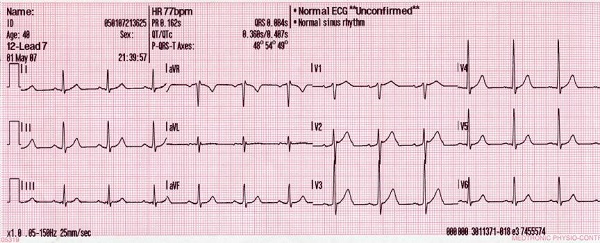 ECG
ECG
Your doctors will want to make a diagnosis quickly. The first test you will have is an ECG tracing of your heart. This should be done within 10 minutes of arriving at hospital. If this shows the characteristic features of a heart attack, a raised ST segment on the ECG, you are likely to be considered for thrombolytic therapy. This type of heart attack is called a STEMI (ST elevation myocardial infarction). In many cases however the ECG will not be diagnostic, it may show some abnormalities but further tests will be necessary to confirm the diagnosis. If you have ongoing pain you may get repeated ECGs.
 Cardiac markers
Cardiac markers
Cardiac markers are used in the diagnosis of a suspected heart attack. These are blood tests that measure chemicals released from the heart muscle following injury. They are very sensitive and specific to heart muscle damage. The cardiac troponins, in particular, have become the cardiac markers of choice for patients with a suspected heart attack. Both the American and European guidelines for diagnosing heart attacks have the measurement of troponin as a key factor. A patient with an elevated troponin level without the classical ECG changes is said to have a non-STsegment elevation MI (NSTEMI). In most hospitals the troponin level with be measured on arrival at the emergency departmant and again a few hours later, but interestingly the recent American (ACC) guidelines state that only 1 elevated troponin level above the established cutoff is required to establish the diagnosis of acute heart attack. This change was proposed following the introduction of increasingly sensitive and precise troponin assays. Up to 80% of patients with acute heart attack will have an elevated troponin level within 2-3 hours of emergency department (ED) arrival.
What it could be
 Chest pain is a common symptom and is always taken seriously, but there are many conditions other than heart attacks that can cause chest pain, these are just a few.
Chest pain is a common symptom and is always taken seriously, but there are many conditions other than heart attacks that can cause chest pain, these are just a few.
- Indigestion
- Angina
- Pulmonary embolus
- Chest infection
- Pleurisy
- Pericarditis (inflammation of the covering of the heart)
- Hyperventilation syndrome
- Reflux

Leave a Reply